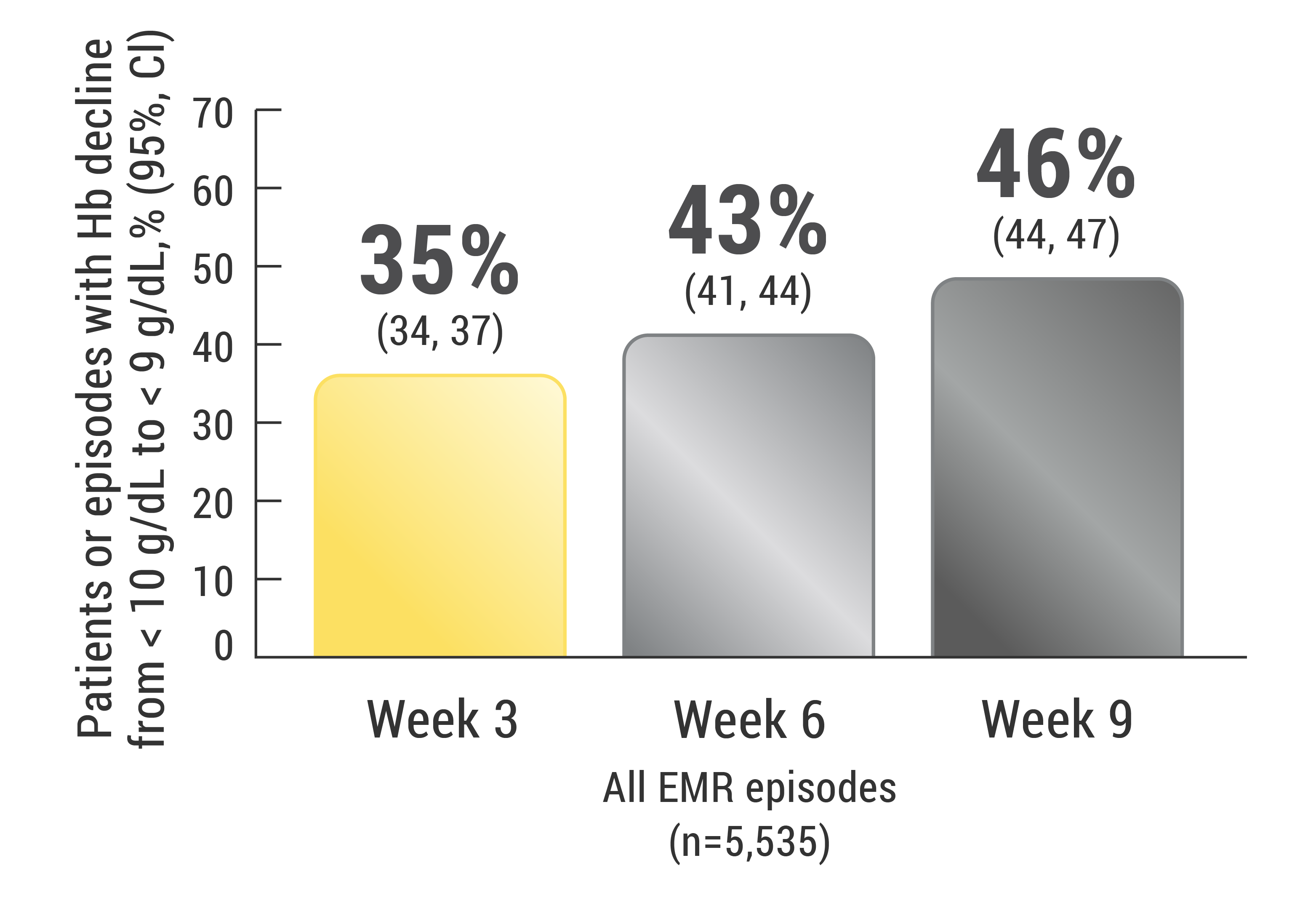
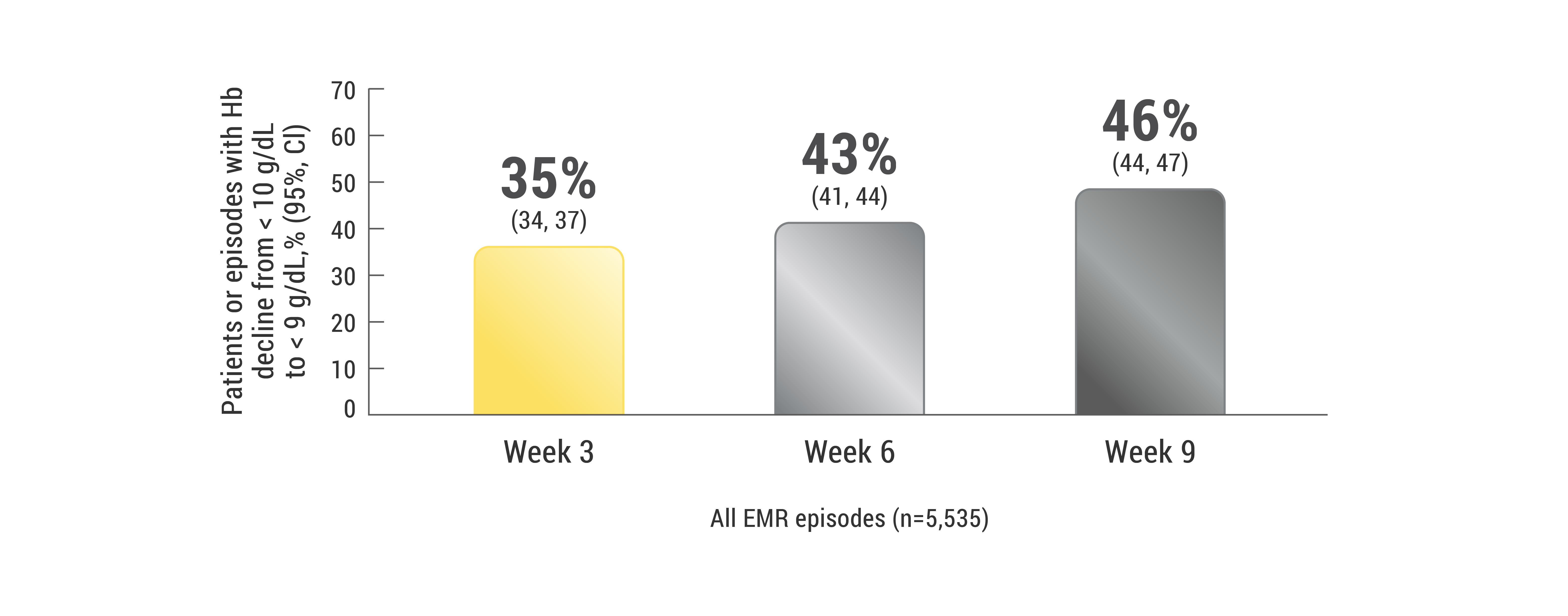
Data are from an aggregated US community oncology clinic electronic medical record (EMR) database of 10,523 patients (representing 10,942 chemotherapy episodes). Patients were at least 18 years of age with non-myeloid malignancies and baseline Hb ≥ 10 g/dL and < 11 g/dL on or after the start of the chemotherapy episode. Patients were treated with a myelosuppressive chemotherapy doublet and could not have received an ESA within 9 weeks before the baseline Hb measurement or at any time during the 18-week study unless Hb was < 9 g/dL. Patients could be in any cycle of their chemotherapy regimen as long as they received at least 2 additional cycles at 35-day intervals after baseline Hb measurement. Chemotherapy episodes were re-indexed when the Hb level was < 10 g/dL to estimate the proportions of episodes and patients that further declined to hemoglobin < 9 g/dL by 3, 6, and 9 weeks without ESA therapy. The total number of EMR episodes with Hb decline from < 10 g/dL to < 9 g/dL was 5,535.1
Adapted with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Cancer and Chemotherapy-Induced Anemia V.2.2017. © 2016 National Comprehensive Cancer Network, Inc. All rights reserved. The NCCN Guidelines® and illustrations herein may not be reproduced in any form for any purpose without the express written permission of NCCN.org. The NCCN Guidelines® are a work in progress that may be refined as often as new significant data becomes available.
The NCCN Guidelines® are a work in progress that may be refined as often as new significant data becomes available. The NCCN Guidelines® are a statement of consensus of its authors regarding their views of currently accepted approaches to treatment. Any clinician seeking to apply or consult any NCCN Guidelines® is expected to use independent medical judgment in the context of individual clinical circumstances to determine any patient’s care or treatment. The National Comprehensive Cancer Network makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
Aranesp® is indicated for the treatment of anemia in patients with non-myeloid malignancies where anemia is due to the effect of concomitant myelosuppressive chemotherapy, and upon initiation, there is a minimum of two additional months of planned chemotherapy.
Aranesp® has not been shown to improve quality of life, fatigue, or patient well-being.
Aranesp® is not indicated for use:
Please see Aranesp® full Prescribing Information, including Boxed WARNINGS, and Medication Guide.
See More +
Aranesp® is indicated for the treatment of anemia in patients with non-myeloid malignancies where anemia is due to the effect of concomitant myelosuppressive chemotherapy, and upon initiation, there is a minimum of two additional months of planned chemotherapy.
Aranesp® has not been shown to improve quality of life, fatigue, or patient well-being.
Aranesp® is not indicated for use:
Please see Aranesp® full Prescribing Information, including Boxed WARNINGS, and Medication Guide.